
The critical need to accelerate cerebral palsy research with consumer engagement, global networks, and adaptive designs
Abstract
The prevalence of cerebral palsy (CP) varies globally, with higher rates and burden of disease in low- and middle-income countries. CP is a lifelong condition with no cure, presenting diverse challenges such as motor impairment, epilepsy, and mental health disorders. Research progress has been made but more is needed, especially given consumer demands for faster advancements and improvements in the scientific evidence base for interventions. This paper explores three strategies to accelerate CP research: consumer engagement, global clinical trial networks, and adaptive designs. Consumer engagement involving individuals with lived experience enhances research outcomes. Global clinical trial networks provide efficiency through larger and more diverse participant pools. Adaptive designs, unlike traditional randomized controlled trials, allow real-time modifications based on interim analyses, potentially answering complex questions more efficiently. The establishment of a CP Global Clinical Trials Network, integrating consumer engagement, global collaboration, and adaptive designs, marks a paradigm shift. The Network aims to address consumer-set research priorities. While challenges like ethical considerations and capacity building exist, the potential benefits for consumers, clinicians, researchers, and funding bodies are substantial. This paper underscores the urgency of transforming CP research methodologies for quicker translation of novel treatments into clinical practice to improve quality of life for those with CP.
1Introduction
Cerebral palsy (CP) is the most common childhood-onset physical disability, with a prevalence ranging from 1.6–3.4 per 1000 live births depending on World Bank Country Income classification [1]. It is evident from the available data that there is a higher prevalence and burden of disease in low- and middle-income countries (LMICs) [1]. CP is life-long with no known cure. Co-morbidities and co-occurring functional limitations are common and can be as disabling as the motor impairment at the core of the diagnosis. Examples include musculoskeletal conditions, epilepsy, chronic pain, sleep disorders, intellectual disability, executive dysfunction problems, dysphagia, mental health disorders, and communication impairments [2]. The severity of physical disability varies from independent ambulation (Gross Motor Function Classification System [GMFCS] levels I–II), to ambulation with aides (GMFCS III), to requiring wheelchairs for mobility (GMFCS IV–V). Individuals with severe physical disabilities require complex medical care. The physical, psychosocial, and economic costs of CP are substantial for people with CP, their families and carers, as well as the communities in which they live. One study estimated that the total financial cost of CP in Australia in 2018 alone was $3.4 billion USD ($5.17B AUD), or $97K USD ($145K AUD) per person (averaged across all levels of physical disability) [3]. A United States-based study estimated the lifetime costs of CP at $921,000 USD in 2003, which has been estimated to equate to over $1.6 million USD in 2023 when adjusted for inflation [4]. Once productivity losses and additional costs outside of health care needs are included, the numbers become even more staggering [5].
In the last decade, momentous research progress has been made in the field of CP, including a 40% reduction in incidence in a high-income context, a reduction in the severity of the physical disability, the discovery of genetic causal pathways, and earlier diagnosis [1, 6, 7]. Despite this, more research is needed and warranted. In a review of interventions for CP, more than 180 different treatments were identified, with only a small fraction of these proven effective through high-quality clinical trials. In fact, 134 of these interventions still require high-quality evidence of efficacy from clinical trials to produce certainty of treatment effects with an estimated cost of $2 billion USD [7]. People with CP want and demand faster research progress [8, 9]. Given this consumer priority and the number of CP interventions available, there is a clear need for more efficient solutions to accelerate the pace of CP research.
Known effective research acceleration strategies include (1) consumer engagement, (2) global research networks, and (3) adaptive trial designs [10–14]. Global networks and adaptive designs are used in other fields, particularly in oncology, with profound benefits to consumers [15]. The aims of this article are to review (1) three known research acceleration solutions, (2) the corresponding evidence base and impact on consumers, and (3) the implications for the CP field in developing and launching a CP global clinical trials network.
2Research acceleration via consumer engagement
Rationale: Consumer engagement is “an informed dialogue between an organisation and consumers, carers and the community which encourages participants to share ideas or options and undertake collaborative decision making, sometimes as partners.” [10] Consumer engagement is founded on the principles of healthcare equity and that people have the right to contribute to decisions that will affect them [10]. It has been known for over a decade that patient and public involvement (PPI) in research, also referred to as consumer engagement, enhances the prioritization, funding, conduct, and utilization of research [16]. People with lived experience have unique insights, the most to gain from contributing to research advancements, and the most to lose from poorly conducted research [16].
Evidence Base and Impact: Systematic reviews confirm that consumer engagement within research is consistently feasible but not always done [10, 17, 18]. Challenges exist to avoid tokenism, including finding a common language, taking extra time, training consumers and researchers, and identifying ways to acknowledge and compensate consumers for their time and expertise [19]. None of these barriers are insurmountable and the benefits outweigh the effort. For example, consumer co-investigators in clinical trials produce statistically faster enrollment rates, which means faster answers for patients [20]. A recent systematic review of 23 randomized controlled trials (RCTs) involving 136,265 participants found evidence that consumer engagement led to (1) enhanced patient outcomes, including improved neonatal survival, (2) production of information that was more relevant, readable, and comprehensible for consumers, (3) identification of a broader range of health care priorities, and (4) improved perceptions of quality of life [10].
Implications for CP: People with CP and their families have clearly articulated several research priorities in research prioritization studies. While the priorities vary among individual people and jurisdictions, they can be broadly grouped into topic areas including etiology, prevention, early diagnosis, early intervention, safe and effective interventions across the lifespan, assistive technologies, novel brain repair agents, natural history and aging, quality of life, participation, and inclusive social policy [9, 21–26]. The list of research priorities is extensive and warrants continued attention and funding. Several consumer councils exist for authentically partnering with people with lived experience to address their research questions (e.g., CP Quest https://cerebralpalsy.org.au/get-involved-research/cp-quest/). As a field, we predominantly conduct small pilot trials in single locations and often unwittingly duplicate existing studies, resulting in research waste and delays in answering consumer priority questions. Engaged partnerships with consumers to co-design and co-lead the next wave of CP research are essential and in place [7].
3Research acceleration via global clinical trial networks
Rationale: “Clinical Trials Networks are collaborative groups of practicing clinician researchers (often several hundred per network) that come together to identify important clinical questions and design large multi-centre clinical trials to answer them” [27]. Known benefits of global clinical trial networks include:
• bringing global attention to an issue,
• access to larger participant pools that create efficiency by accelerating clinical trial enrollment and completion rates to benefit patients sooner,
• inclusion of diverse patient populations that enhance generalizability and applicability,
• cost-effectiveness through shared infrastructure and resources,
• increased access to specialized expertise,
• more rapid translation of trial results into clinical practice [11, 28].
These benefits arise from the commitment and engagement of a large group of practicing clinicians navigating various regulatory environments [12].
Evidence Base and Impact: One of the best-known examples of utilizing the power of global clinical trial networks to improve patient outcomes is the field of pediatric oncology (e.g., Children’s Oncology Group). For decades, pediatric oncology has tested novel treatments in rare populations and then translated findings into usual care, lifting the rate of five-year survival from 73% to 87% in Australia (1983–2018) and 58% to 85% in the United States (mid-1970s to 2023) [15, 29]. Another example of a successful network is the PEDSnet network which utilizes the power of big data, with pre-approved electronic medical records data on more than 9 million children across multiple pediatric hospitals. Since its inception, PEDSnet has been awarded over $125 million USD in competitive grant funds and published 91 studies [30].
Implications for CP: Multiple excellent research networks already exist in the CP field, such as the American collaborative known as the CP Research Network (CPRN, https://cprn.org), CHILD-BRIGHT in Canada (https://www.child-bright.ca), and the Australasian Cerebral Palsy Clinical Trials Network (https://cre-auscpctn.centre.uq.edu.au). However, these are predominantly single-country networks. The next logical step is a global research network. The CP field has witnessed the positive outcomes of global clinical trials generating impactful research, particularly in neonatology. A notable example involves the administration of magnesium sulfate to mothers in preterm labor, demonstrating a protective effect against CP (relative risk [RR] 0.68, 95% confidence interval [CI] 0.54–0.87, n = 4601 babies, five trials, number needed to treat [NNT] to benefit 46) [31]. This achievement was realized through collaborative global multi-center clinical trials facilitated within a neonatal network. These trials were then aggregated in an individual participant data meta-analysis [31]. The subsequent widespread integration of magnesium sulphate into usual care is believed to have contributed to the observed 40% reduction in the incidence of CP in Australia [6].
4Research acceleration via adaptive designs
Rationale: Conventional fixed RCTs are considered the pinnacle methodology for confirming the efficacy of a treatment; however, their limitations are well-documented [32]. RCTs do not consider individual preferences, differential adherence, attrition, or tailoring of an intervention to an individual. There is no real-time assessment of data as it is captured to recalculate a sample size, adjust subject allocation, or even adapt the research question itself. Further, conventional trials can only ask one research question at a time. They are slow and sequential, prohibitively costly, and labor-intensive [32]. Recruitment issues in traditional clinical trials are also common, resulting in underpowered studies that cannot provide definitive answers and are limited in their generalizability [33]. This is particularly problematic in locations of lower population density (e.g., Australia).
In response to the challenges outlined above, and because of advances in statistics, innovative clinical trial designs have emerged in various fields such as oncology and intensive care medicine (e.g., REMAP-CAP) [34]. Specific questions lend themselves to adaptive designs, including the assessment of which drugs are more effective, in what combination and sequence, at what dose and duration, and for which sub-groups. In contrast to conventional RCTs, trials using adaptive designs offer a more flexible and efficient approach to clinical research, allowing for pre-planned, within trial modifications to trial and/or statistical procedures based on interim analyses of accumulated data. These modifications follow tightly defined, a priori rules and decision-making criteria to ensure scientific integrity is not compromised [14]. Adaptive designs allow for multiple arms and heterogeneous study populations (e.g., basket, umbrella, and platform trials). Particularly when combined with Bayesian statistical approaches, adaptive designs have the potential to improve study power, reduce sample size and total cost, and shorten time for drug development and testing of novel interventions for CP [13, 14].
Implications for CP: Adaptive designs herald a new era for CP research, potentially answering complex clinical questions that to date have proven challenging for the traditional RCT. Instead of conducting multiple single-site pilot trials with inconclusive results, the use of innovative trial designs could significantly increase the field’s capacity to definitively answer priority research questions for people with CP in a timely way. See Fig. 1 for examples of how adaptive designs can be applied to CP.
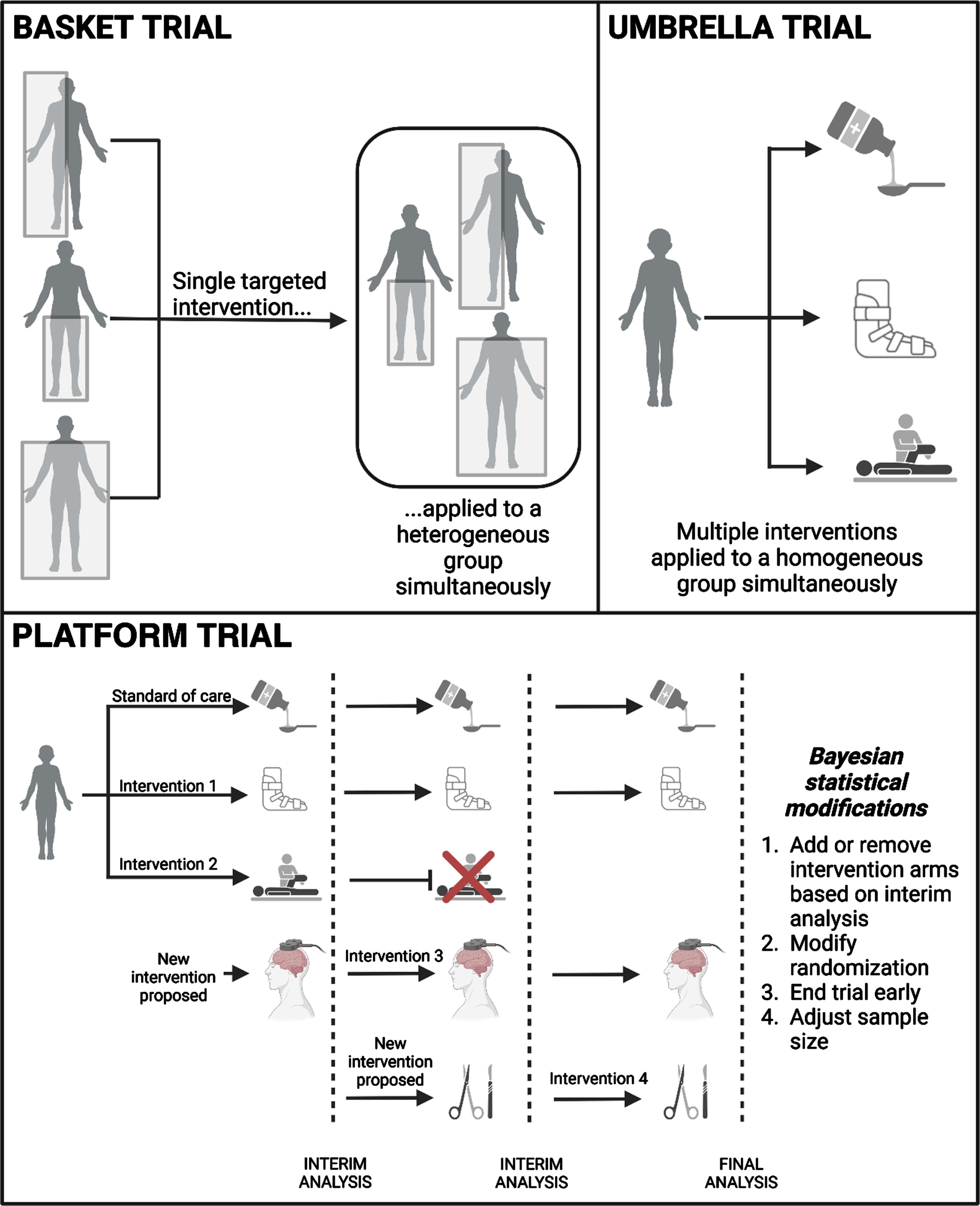
Fig. 1
Types of adaptive designs. Here we review three adaptive designs and show how they can be applied directly to CP. Basket trials classically test one intervention in multiple diseases. In CP, we can instead test different phenotypes (shown here), etiologies, or types of muscle tone. Umbrella trials allow multiple intervention arms to be tested simultaneously, shown here as a medication, bracing, and therapy. Finally, platform trials allow for the greatest flexibility, with one control group receiving the standard of care (e.g., enteral medicine) and others receiving test interventions simultaneously (e.g., bracing, therapy, transcranial magnetic stimulation, and surgery). The addition of Bayesian statistical models further customizes the trial, reducing costs and total time to investigate all study interventions. (Created with BioRender.com).
5Types of trials using adaptive designs
The idea of a trial master protocol has emerged in response to the need for more efficient RCTs with the ability to evaluate multiple treatments across multiple patient types [35]. A master protocol is an overarching protocol for a collection of trials or sub-studies, designed to address multiple research questions. Three common trial designs which may be governed by a master protocol include basket trials, umbrella trials, and adaptive platform trials (APTs). However, it should be noted that each adaptive trial should be designed in a bespoke manner according to the needs and constraints of the individual context, as opposed to fitting a trial to a pre-defined category.
Basket Trials: A basket trial involves investigating the efficacy of one intervention for participants across multiple conditions or sub-types of a particular disease. In oncology, for instance, a basket trial may evaluate the effect of a specific treatment targeting a particular gene mutation that is shared by multiple cancer phenotypes (e.g., BRAF V600); statistical models may be used to ‘borrow’ information about treatment effects across the various cancer types. In CP, the concept of different “conditions” could be extended to different CP motor sub-types, facilitating greater inclusion of participants with rarer CP sub-types into research studies. Master protocols governing basket trials can specify the patient sub-types (strata) for which subtype-specific effects will be estimated, as well as the average efficacy across all sub-types [36].
Umbrella Trials: Umbrella trials involve investigating the efficacy of multiple interventions for participants with a single, specific condition, disease, or patient subtype. The multiple interventions can be tested against a common control arm or alternatively compared against each other. Given the vast array of interventions for CP, there is a clear need to investigate their efficacy more efficiently than could be done in a conventional RCT in which only one intervention is tested at a time.
APTs: An APT describes a trial run in a continuous manner, with new arms entering and exiting the study based on pre-defined criteria [14]. APTs combine the focus of umbrella trials on evaluating multiple interventions simultaneously with the focus of basket trials on evaluating interventions across multiple patient subtypes, with the overall objective of determining the best treatment strategy for a complex condition with multiple patient subtypes (e.g., people with CP). The master protocol defines the patient subtypes, which are the basis of treatment eligibility and stratum-specific randomization. As an APT progresses, pre-planned interim analyses of accumulating study data may trigger the end of a specific study arm and inform updates to randomization allocation, using trial resources as efficiently as possible. This will be particularly beneficial for studies in rarer sub-types of CP in which the sample size will be limited, providing definitive answers to complex questions that previously remained unanswered.
5.1Ethical considerations
Autonomy: Robust debate has surrounded the ethical challenges of adaptive designs as uptake has increased. The question arises: do adaptive designs offer ethical advantages over fixed RCTs, or in essence, create fresh concerns? While most experts would likely agree that adaptive designs are more efficient, it is their complexity that causes tension. Complexity impacts respect for persons, specifically valid informed consent and subsequent threats to the key principle of autonomy [37]. After all, if considerations of adaptive design components are highly complex for an institutional review board, how much more confusing may the process seem to a layperson? [14] Several solutions have been proposed regarding consent practices, with skilled communication at the heart of all the approaches. Strategies to enhance participant understanding could utilize multimedia and increase the time allocated for consenting processes. From the beginning, patient information sheets should outline each stage’s possible modifications, with updates provided when, for example, an intervention arm is dropped [38]. Participant information sheets must openly explain the ‘broad’ nature of consent required in adaptive designs (compared to ‘specific’ consent in a RCT), transparently forecast that later entry participants may receive more benefit (compared to starting recruits), and disclose that there may be differing interventions offered to individuals as the trial progresses [39]. Consumers will be essential in co-designing explanatory participant information sheets and visuals to ensure that potential participants understand what they are consenting to.
Beneficence: Both efficiency and prospective participant benefit are reasons for preferring adaptive designs over RCTs [37]. However, the disruption of clinical equipoise from data accrual and ongoing modifications to intervention arms is challenging for some participants and clinicians. Beneficence may be afforded in greater measure to adaptive design participants due to the tailoring of the trial design to the patient’s disorder, the ability to transition to intervention arms showing more benefit, and the overall time saved. As ongoing trial adaptations optimize the interventions received, treatment risks are lowered [39]. Ethical threats created by adaptive designs are manageable but require authentic consumer engagement at every stage of the research cycle. Researchers in this new frontier will need to listen well.
Justice: The geographical distribution of clinical trials has shifted to LMICs and emerging economies where costs are lower, markets are expanding, and participants are plentiful and more easily recruited [40]. This is positive as under-represented populations are now included within research. However, adequate regulatory oversight is essential for protecting the rights and interests of research participants and maintaining partnership equity [41]. Concerns have arisen in LMICs where clinical trial governance and regulatory systems and processes are not yet aligned with global standards. In response, some LMICs have introduced stringent regulatory protections for clinical trial participants [40]. Thus, research is becoming more challenging to undertake in some LMICs because of complex trial regulations and increased administrative burdens. It is a balancing act between providing necessary protections for research participants and potentially depriving local populations of the benefits of research, such as the opportunity to access novel treatments via clinical trials [40].
The rate of CP is almost three times higher in LMICs compared to high-income countries (HICs; 3.4/1000 vs. 1.6/1000) [1]. The burden of disease is also higher. Non-ambulant CP is the most common presentation in LMICs and wheelchairs are often unavailable, whereas ambulant CP is the most common presentation in HICs. This uneven burden of disease needs to be addressed by conducting more research in these locations. Research needs to consider adopting known effective interventions that reduce the incidence of CP, as well as novel treatments for those living with CP. Feasibility, affordability, and responsivity to treatment in the presence of severe brain injury all need to be carefully considered.
6Consumer co-designed, network-led international adaptive clinical trials: The ultimate frontier
In response to consumer demand and in alignment with the evidence for best-practice consumer engagement, global clinical trial networks, and adaptive designs, a CP Global Clinical Trials Network has now been established. The Network proposes a major paradigm shift in how global CP research is conducted to improve outcomes and the quality of life for people living with CP by harnessing innovative adaptive designs and big data to expedite the conduct of CP clinical trials. It is an international collaboration of people with CP, researchers, and clinicians committed to transforming the landscape of CP research. The ultimate aim is for everyone with CP, no matter where they live, to have access to cutting-edge clinical trials and the rapid translation of novel effective treatments into usual clinical practice. The Network has a strong central leadership team that integrally includes people with CP. In the establishment phase, a modified Delphi survey was conducted, and there was consensus that the Network should involve people with CP at all stages of research, embrace a consumer reference group, and primarily seek to address the consumer-set research priorities described in the literature [42]. To facilitate global collaboration and inclusivity, the CP Global Clinical Trials Network is building a shared infrastructure with collective expertise to handle complex clinical trials in all income contexts, led by world-leading statisticians with expertise in Bayesian statistics and adaptive designs. A critical part of this plan includes capacity building in the CP field in this emergent methodology [43].
Harnessing innovative designs will make CP research more efficient, fairer for participants, and more easily translatable into clinical care. Direct beneficiaries include people with CP, clinicians, researchers, and funding bodies. People with CP, especially those within the rarer subgroups, will be the ultimate beneficiaries because they will have faster access to new treatments that produce real benefits. With adaptive trial methodologies, participants are more likely to be assigned to a more effective treatment. Clinicians will gain faster access to cutting-edge protocols for the most effective treatments, enabling them to provide state-of-the-art care to individuals with CP. Researchers will benefit because adaptive trial methodologies optimize the allocation of participants, ensuring more efficient and impactful research, reducing redundancies, and maximizing the potential for new discoveries. Funding bodies will benefit because costs are lowered and research waste is reduced, increasing the return on investment. In addition, commercial sponsors may be more willing to invest in CP trials that allow for modifications based on accumulating data, allowing for increased feasibility and faster testing of novel treatments.
To succeed, there needs to be a critical investment in network infrastructure and capacity building of the clinical trials workforce. Low levels of familiarity and expertise in adaptive designs among stakeholders are key challenges. However, more educational and funding opportunities are emerging thanks to targeted advocacy campaigns (e.g., by the Australian Clinical Trials Alliance), funders, and regulatory bodies (e.g., the National Institutes of Health and Food and Drug Administration in the United States) increasingly recognizing the need for innovative trial designs. Awareness is growing around the critical need to invest in capacity building and infrastructure for the conduct of global multi-center adaptive trials.
7Conclusions
Our current approach to conducting clinical trials in CP leaves families, clinicians, researchers, and policymakers still searching for answers. To meet these needs, the CP field requires a transformative shift in how we approach research. We have a significant opportunity to reshape the landscape of disability research, with crucial implications for advancing the health and well-being of people with disabilities through the newly established CP Global Clinical Trials Network, funded by philanthropy. In line with recommendations from scientific literature, the CP Global Clinical Trials Network aims to definitively address the complex questions that are most important to people with CP.
Acknowledgments
We wish to gratefully acknowledge the vision and leadership of the Elsass Foundation Denmark (#23-C01-0980) and the Cerebral Palsy Alliance Australia (#PRG09521) for providing the philanthropic funding to establish the CP Global Clinical Trials Network.
Conflict of interest
Sruthi P. Thomas – employed by Baylor College of Medicine.
Iona Novak – employed by The University of Sydney.
Anina Ritterband-Rosenbaum – employed by the Elsass Foundation, Denmark.
Karin Lind – employed by the University of Sydney.
Annabel Webb – employed by Cerebral Palsy Alliance, Australia.
Paul Gross – none.
Maria McNamara – employed by Cerebral Palsy Alliance, Australia.
references
[1] | McIntyre S , Goldsmith S , Webb A , et al. Global prevalence of cerebral palsy: A systematic analysis. Dev Med Child Neurol. (2022) ;64: (12):1494–506. doi: 10.1111/dmcn.15346 |
[2] | Hollung SJ , Bakken IJ , Vik T , et al. Comorbidities in cerebral palsy: A patient registry study. Dev Med Child Neurol. (2020) ;62: (1):97–103. doi: 10.1111/dmcn.14307 |
[3] | The cost of cerebral palsy in Australia in 2018. Canberra: Deloitte Access Economics; 2019. Available from: https://cerebralpalsystrategy.com.au/wp-content/uploads/2020/02/DAE_Cost-of-cerebral-palsy-in-2018_FINAL.pdf |
[4] | Centers for Disease Control and Prevention. Economic costs associated with mental retardation, cerebral palsy, hearing loss, and vision impairment. MMWR Morb Mortal Wkly Rep. (2004) ;53: :57–9. |
[5] | Tonmukayakul U , Shih STF , Bourke-Taylor H , et al. Systematic review of the economic impact of cerebral palsy. Res Dev Disabil. (2018) ;80: :93–101. doi: 10.1016/j.ridd.2018.06.012 |
[6] | Australian Cerebral Palsy Register Report 2023. Sydney: Australian Cerebral Palsy Research Institute; 2023. Available from: https://cpregister.com/wp-content/uploads/2023/01/2023-ACPR-Report.pdf |
[7] | Novak I , Morgan C , Fahey M , et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr Neurol Neurosci Rep. (2020) ;20: (2):3. doi: 10.1007/s11910-020-1022-z |
[8] | The Lancet Neurology. People with cerebral palsy demand a major shift in research. Lancet Neurol. (2023) ;22: (2):101. doi: 10.1016/S1474-4422(23)00006-6 |
[9] | Lungu C , Hirtz D , Damiano D , Gross P , Mink JW . Report of a workshop on research gaps in the treatment of cerebral palsy. Neurology. (2016) ;87: (12):1293–8. doi: 10.1212/WNL.0000000000003116 |
[10] | Wiles LK , Kay D , Luker JA , et al. Consumer engagement in health care policy, research and services: A systematic review and meta-analysis of methods and effects. Gholipour K, editor. PLoS One. (2022) ;17: (1):e0261808. doi: 10.1371/journal.pone.0261808 |
[11] | Nemeh F , Buchbinder R , Hawley CM , Nelson MR , Waterkeyn JG , Reid CM . Activities supporting the growth of Clinical Trial Networks in Australia. Trials. (2022) ;23: (1):81. doi: 10.1186/s13063-021-05974-3 |
[12] | Thomas KS , Koller K , Foster K , Perdue J , Charlesworth L , Chalmers JR . The UK clinical research network – has it been a success for dermatology clinical trials? Trials. (2011) ;12: (1):153. doi: 10.1186/1745-6215-12-153 |
[13] | Weir CJ . Adaptive clinical trials and their potential to improve drug-development efficiency. Clin Investig (Lond). (2015) ;5: (4):359–61. doi: 10.4155/cli.14.134 |
[14] | The Adaptive Platform Trials Coalition. Adaptive platform trials: Definition, design, conduct and reporting considerations. Nat Rev Drug Discov. (2019) ;18: (10):797–807. doi: 10.1038/s41573-019-0034-3 |
[15] | Siegel RL , Miller KD , Wagle NS , Jemal A . Cancer statistics, 2023. CA Cancer J Clin. (2023) ;73: (1):17–48. doi: 10.3322/caac.21763 |
[16] | Brett L , Siette J , Nguyen A , et al. At the grassroots of home and community-based aged care: Strategies for successful consumer engagement. BMJ Open. (2019) ;9: (11):e028754. doi: 10.1136/bmjopen-2018-028754 |
[17] | Domecq JP , Prutsky G , Elraiyah T , et al. Patient engagement in research: A systematic review. BMC Health Serv Res. (2014) ;14: (1):89. doi: 10.1186/1472-6963-14-89 |
[18] | Biddle MSY , Gibson A , Evans D . Attitudes and approaches to patient and public involvement across Europe: A systematic review. Health Soc Care Community. (2021) ;29: (1):18–27. doi: 10.1111/hsc.13111 |
[19] | Price A , Albarqouni L , Kirkpatrick J , et al. Patient and public involvement in the design of clinical trials: An overview of systematic reviews. J Eval Clin Pract. (2018) ;24: (1):240–53. doi: 10.1111/je12805 |
[20] | Crocker JC , Ricci-Cabello I , Parker A , et al. Impact of patient and public involvement on enrolment and retention in clinical trials: Systematic review and meta-analysis. BMJ. (2018) ;363: :k4738. doi: 10.1136/bmj.k4738 |
[21] | Australian and New Zealand Cerebral Palsy Strategy 2020. Australian and New Zealand Cerebral Palsy Strategy Collaboration; 2020. Available from: https://cpstrategy.wpengine.com/wp-content/uploads/2020/03/CP-Strategy-BOOKLET-2020_WEB_FINAL_V2.pdf |
[22] | Gilbert LA , Fehlings DL , Gross P , et al. Top 10 Research Themes for Dystonia in Cerebral Palsy. Neurology. (2022) ;99: (6):237–45. doi: 10.1212/WNL.0000000000200911 |
[23] | Gross PH , Bailes AF , Horn SD , Hurvitz EA , Kean J , Shusterman M . Setting a patient-centered research agenda for cerebral palsy: A participatory action research initiative. Dev Med Child Neurol. (2018) ;60: (12):1278–84. doi: 10.1111/dmcn.13984 |
[24] | Childhood Neurological Conditions Top 10 Priorities. James Lind Alliance; 2024. Available from: https://www.jla.nihr.ac.uk/priority-setting-partnerships/childhood-neurological-conditions/top-10-priorities.htm |
[25] | Mcintyre S , Novak I , Cusick A . Consensus research priorities for cerebral palsy: A Delphi survey of consumers, researchers, and clinicians. Dev Med Child Neurol. (2010) ;52: (3):270–5. doi: 10.1111/j.1469-8749.2009.03358.x |
[26] | Wu YW , Mehravari AS , Numis AL , Gross P . Cerebral palsy research funding from the National Institutes of Health, 2001 to 2013. Dev Med Child Neurol. (2015) ;57: (10):936–41. doi: 10.1111/dmcn.12789 |
[27] | What is a clinical trials network? Melbourne: Australian Clinical Trials Alliance; 2024. Available from: https://clinicaltrialsalliance.org.au/about-acta/clinical-trials-network/ |
[28] | The joint ACTA/ACSQHC Working Group. The value proposition of investigator-initiated clinical trials conducted by networks. Med J Aust. (2021) ;214: (4):159–61. doi: 10.5694/mja2.50935 |
[29] | Cancer Data in Australia. Australian Institute of Health and Welfare; 2023 [updated 31 August 2023]. Available from: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia/contents/about |
[30] | PEDSnet [homepage on the internet]. PEDSnet. Available from: https://pedsnet.org/ |
[31] | Crowther CA , Middleton PF , Voysey M , et al. Assessing the neuroprotective benefits for babies of antenatal magnesium sulphate: An individual participant data meta-analysis. PLoS Med. (2017) ;14: (10):e1002398. doi: 10.1371/journal.pmed.1002398 |
[32] | Hariton E , Locascio JJ . Randomised controlled trials – the gold standard for effectiveness research. BJOG An Int J Obstet Gynaecol. (2018) ;125: (13):1716–1716. doi: 10.1111/1471-0528.15199 |
[33] | Kadam R , Borde S , Madas S , Salvi S , Limaye S . Challenges in recruitment and retention of clinical trial subjects. Perspect Clin Res. (2016) ;7: (3):137. doi: 10.4103/2229-3485.184820 |
[34] | Angus DC , Berry S , Lewis RJ , et al. The REMAP-CAP (Randomized Embedded Multifactorial Adaptive Platform for Community-acquired Pneumonia) Study. Rationale and Design. Ann Am Thorac Soc. (2020) ;17: (7):879–91. doi: 10.1513/AnnalsATS.202003-192SD |
[35] | Woodcock J , LaVange LM . Master Protocols to Study Multiple Therapies, Multiple Diseases, or Both. N Engl J Med. (2017) ;377: (1):62–70. doi: 10.1056/NEJMra1510062 |
[36] | Hyman DM , Puzanov I , Subbiah V , et al. Vemurafenib in Multiple Nonmelanoma Cancers with BRAF V600 Mutations. N Engl J Med. (2015) ;373: (8):726–36. doi: 10.1056/NEJMoa1502309 |
[37] | Chongwe G , Ali J , Kaye DK , Michelo C , Kass NE . Ethics of Adaptive Designs for Randomized Controlled Trials. Ethics Hum Res. (2023) ;45: (5):2–14. doi: 10.1002/eahr.500178 |
[38] | Pallmann P , Bedding AW , Choodari-Oskooei B , et al. Adaptive designs in clinical trials: Why use them, and how to run and report them. BMC Med. (2018) ;16: (1):29. doi: 10.1186/s12916-018-1017-7 |
[39] | Paul NW , Mahdiani H . Ethical challenges in clinical studies with adaptive design in oncology. Clin Ethics. (2023) ;18: (2):148–54. doi: 10.1177/14777509221133974 |
[40] | Aguilera B , DeGrazia D , Rid A . Regulating international clinical research: An ethical framework for policy-makers. BMJ Glob Heal. (2020) ;5: (5):e002287. doi: 10.1136/bmjgh-2020-002287 |
[41] | Modlin C , Sugarman J , Chongwe G , et al. Towards achieving transnational research partnership equity: Lessons from implementing adaptive platform trials in low- and middle-income countries. Wellcome Open Res. (2023) ;8: :120. doi: 10.12688/wellcomeopenres.18915.2 |
[42] | Novak I , Fahey M , Dan B , et al. CP Global Clinical Trials Network, an International Trials Network for Cerebral Palsy: Global Prioritisation Process Using the Modified Delphi Method. SSRN; 2024. Available from: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4681864 |
[43] | Kairalla JA , Coffey CS , Thomann MA , Muller KE . Adaptive trial designs: A review of barriers and opportunities. Trials. (2012) ;13: (1):145. doi: 10.1186/1745-6215-13-145 |

